Know your
Inflammatory Back-Ache/Arthritis
by Dr LATA BICHILE
Every individual suffers from backache in his or her life time. Nature of it is either acute, subacute or chronic. This write will focus on sub acute to chronic back pain occurring in patients below the age of 40 years.
Pain characteristics are either severe and do not permit movement at all. It could all be a lancinating type like an electric current and that restricts movement. Few may experience a pain that starts during late night or early morning and associated with stiffness or tightness. Patient finds it difficult to turn on sides during sleep and attempting so disturbs sleep. At times in cold and rainy season or in an AC environment patient is so miserable that he or she seeks help while getting up from bed or from sitting posture.
It has been a common observation that individuals with acute back ache seek medical attention in time and the problem is sorted out. But unfortunately, patients with subacute back ache of more than 6 weeks to few months postpone evaluation by experts and attribute to heavy unusual work, prolonged standing, working in AC, leucorrhoea and some minor fall. These categories of young patients are the ones who need evaluation by Rheumatologist to rule out a condition called as Inflammatory Backache or Arthritis of Spine and Bilateral SI joints the joints located beneath both buttocks.
HOW TO RECOGNISE INFLAMMATORY BACK - ACHE The cardinal complaints of such aback ache are as below,
1.Patients are young below the age 40 yrs.
2.Males out number than females.
3.Often there is family history of back pain from maternal or paternal side affecting the male members of the family.
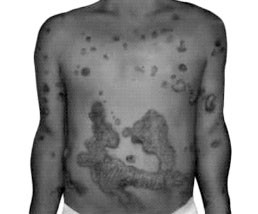
4.On enquiry there is history of Psoriasis, a Chronic inflammatory skin disorder characterised by silver coated skin
lesions over joint areas.
(Refer to Photographs 1 to 4)
5.On enquiry there is history of chronic loose motions with abdominal pain, blood and mucous in stool.
6.The back pain is nocturnal and brings difficulties on turning to sides and disturbs sleep.
7.Back stiffness is so much that patients support back with the hand and need rest before few steps.
8.Patient cannot bend forwards and finds difficult to pick up objects on floor or in a female patient she finds difficult to clean the floor on bending.
9.This stiffness weans off as the day today activities move on. Many patients notice stiffness till 1PM.
10.Patients again notice pain when on sedentary job Or on reaching home and while resting.
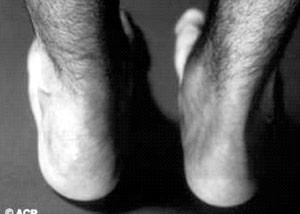
11.Some patients(15 to 20 %) experience heel pain, stiffness, plantar pain , tendo achillitis, sausage digit of a finger or a toe.
12.5 to 10% patients notice anterior uveitis with pain, redness associated with blurred vision.
13.Very often few patients get catch in the chest wall due to costochondritis that mimics Angina
Thus from above symptoms it is evident that the pain and stiffness are the hall mark complaints suggesting Inflammatory disease. These patients need Rheumatologist opinion before the disease takes a natural course of fusion of the joints and leaving patients in misery and disability. We all Rheumatologist come across such patients after 5 to 7 years of disease onset when patient has missed the window of therapeutic opportunities that will reverse the/ Halt the disease process. Such numbers are many verses those reporting early. This scenario can be altered if patients come with a mindset that Arthritis is treatable and they become self-advocates in spreading disease information and treatment benefits.
INVESTIGATIONS
Before planning the treatment, a panel of tests are advocated to assess general health and organ safety. Disease process is chronic and so is the treatment course. Patients and their near ones have to be closely involved in the process of health support, psychosocial, financial, domestic support as is practised in patients with heart attack or Cancer.
COMMON INVESTIGATIONS
CBC, ESR, PLATELETS
CRP
LFT
RFT SERUM CALCIUM, PHOSPHARUS, ALKALINE
PHOSPHATASE
VITAMIN D LEVELS
HLA B27
X RAY OF LS SPINE AND SI JOINTS
SI JOINTS IN PRONE POSITION
MRI SI JOINTS AND LS SPINE USG OF KNEE, SHOULDER, TENDO
ACHILLITIS
X RAY KNEE JOINTS
X RAY CHEST
TREATMENT PLAN
1.Treatment aims at relieving pain and stiffness with pain killers that suit to individual patient.
2.Maintaining posture.
3.Halt disease activity with DMARDS, ANTI TNF Alfa Agents.
4.Encourage exercises of back extensors, Neck, SI joints, Foot.
5.Breathing exercises.
6.Swimming
It is essential that patients follow treatment regularly along with exercises to keep the Spine in Natural position, flexible, pain free. It is advisable as well as beneficial that patients stick to only one type of pathy for the disease i.e. progressive and disabling. Do not mix treatment from all the streams available. Such treatments areimpressed upon by relatives, friends, neighbours. Current allopathic medicines have rational basis & treatment outcome data is available.
Treat to Target Treatment Approach
Go slow and treat low approach is abandoned in Rheumatology practice. So is the treatment of Back Arthritis called as AS or Spondyloarthropathy.
In As target is the TNF Alfa i.e. produced in body that triggers the Inflammation& the disease. Anti TNF drugs belong to Treat to Target category that blocks TNF alfa.
This class of drugs are manufactured in India. These are called as Biosimilars. However, on Efficacy, Safety & Disease Outcome they match with the Innovator. Due to judicious usage of Infections Screening Protocol for Latent Hepatitis & TB, Infections on the usage of Biosimilars/ Innovators has fallen down.
Biosimilars/ Biologicals when administered early in the disease course, the benefit is tremendous versus when administered late. The decision of Institution of these class of drugs is supported by MRI that reveals Bone Marrow Edema, Sufficing Disease Activity vs Joint Arthrosis.
So the patient and the relatives must be inclined to early use in contrast to a stage of spinal fusion or hip joint/ knee joint fusion. These agents are administered as IV infusions or sub cute injections at least for 6 months and then given as and when required. A battery of investigations is performed to rule out prevalent infection as Tb, Hepatitis and then therapy initiated.
With IV injections patients improve in hours and with sub cute injection type patients improve by three weeks and continue to sustain benefit. First line drug Methotrexate/ Sulfasalazine is continued to avoid development of antibodies against Anti TNF agents.
Biological therapy is a job of experts and hence patients should be in the hands of Rheumatologist.
Along with Biological agents' patients are advised to continue pain killers as and when required, to continue exercises and follow healthy life style and diet without any prejudices. Often Calcium, Vit. D are given to maintain Bone Health.
Patients with bad Hip, Knee disease are recommended Joint Replacement Surgery, few patients need Vertebroplasty, Osteotomy.
Currently Heart Attack & Brain Stroke are managed within two golden hours of the onset for a Better outcome. In Rheumatology practise there is no Golden hours but there should be a perception of At least few Golden months (3-6) during which the patients, relatives & the Policy makers should help in the process of decline Disease burden and Improving Quality of Life of Individual patient by Offering Biologicals.
On the Pharma front, All Biosimilars are Efficacious & Economical, so the patients should Invest on their health to remain Disease free & enjoy Quality of Life.
Photograph 1: Patient of Psoriasis with Hand Arthritis

Photograph 2: Sausage Digit Arthritis

Photograph 3: Skin Psoriasis Arthritis
Photograph 4: Tendo Achilitis in Psoriasis Arthritis
Photograph 5: Life with AS Arthritis

Photograph 6 : Ankylosing Spodylitis Arthritis



